
Proposed Medicaid changes could require cost sharing for expansion adults, perhaps burdening older adults and those with chronic conditions. This could especially affect high-needs enrollees, as a new bill in Congress considers shifting the financial landscape of the Affordable Care Act (ACA) Medicaid expansion program. Enrollees between 100% and 138% of the federal poverty level could face up to $35 per service, excluding primary care, mental health, and other crucial services. Research indicates that cost sharing frequently enough reduces access to necessary care. Imagine an older adult facing increased copays for ongoing health issues while a 50-64-year-old single enrollee could pay an astonishing 4.7% of their income. News Directory 3 offers an in-depth analysis of potential cost-sharing impacts based on 2021 Medicaid claims data. Discover what’s next in the debate.
Medicaid Expansion: Cost Sharing Could Burden Older, Sicker Adults
Updated June 27, 2025
A proposed budget bill in Congress could significantly alter Medicaid by mandating cost sharing for certain adults enrolled thru the Affordable Care Act (ACA) Medicaid expansion. This shift contrasts with current regulations that allow, but don’t require, states to implement cost sharing within limits designed to protect enrollees from excessive out-of-pocket expenses.
Research suggests that even small co-payments can hinder access to necessary care for low-income individuals. Cost sharing is linked to reduced healthcare utilization,poorer health outcomes,and increased financial strain. Studies also indicate that cost sharing often yields limited savings for states and can decrease provider reimbursements.
The bill would require states to impose cost sharing of up to $35 per service on Medicaid expansion adults with incomes between 100% and 138% of the federal poverty level (FPL), which is $15,650 for a single adult in 2025. Exempt services include primary care, mental health and substance use disorder (SUD) treatment, family planning, emergency care provided in a hospital emergency department, and institutional long-term care. prescription drug cost sharing would remain at nominal levels, as per existing rules. States can opt to charge less than $35, but providers can still demand payment before providing services, potentially denying care if enrollees cannot pay.
Current rules permit states to impose cost sharing on Medicaid expansion adults, but federal guidelines limit charges based on enrollees’ ability to pay. Maximum allowable cost sharing varies by service type and income, with total out-of-pocket costs capped at 5% of family income. States must track incurred cost sharing and halt it onc the cap is reached, a provision the bill would maintain.Before the COVID-19 pandemic, over half of Medicaid expansion states charged cost sharing for some services. While most states imposed cost sharing irrespective of income, some limited it to adults with incomes at or above 100% FPL. States were barred from introducing or increasing cost sharing from January 2020 through December 2023 in exchange for increased federal Medicaid funding. While states could reimpose cost sharing starting in January 2024, some have since eliminated it entirely.
Because the bill focuses on cost sharing for a specific group of expansion enrollees, it likely won’t affect existing state cost-sharing policies. States currently imposing cost sharing will probably maintain it, potentially applying it to a broader range of services for expansion adults with incomes between 100% and 138% FPL. States with cost-sharing requirements exceeding $35 per service may need to reduce the amount for this population. Cost sharing for other populations can likely remain in place if it complies with existing rules.
An analysis of 2021 Medicaid claims data estimates the potential cost-sharing burden on enrollees if all states imposed maximum amounts. The analysis,which serves to illustrate which enrollees may be subject to the most cost sharing,assumes cost sharing of $35 per non-exempt service. Prescription drug cost sharing, which the bill mandates be limited to nominal amounts, is not included. Many states already charge nominal amounts for prescription drugs.
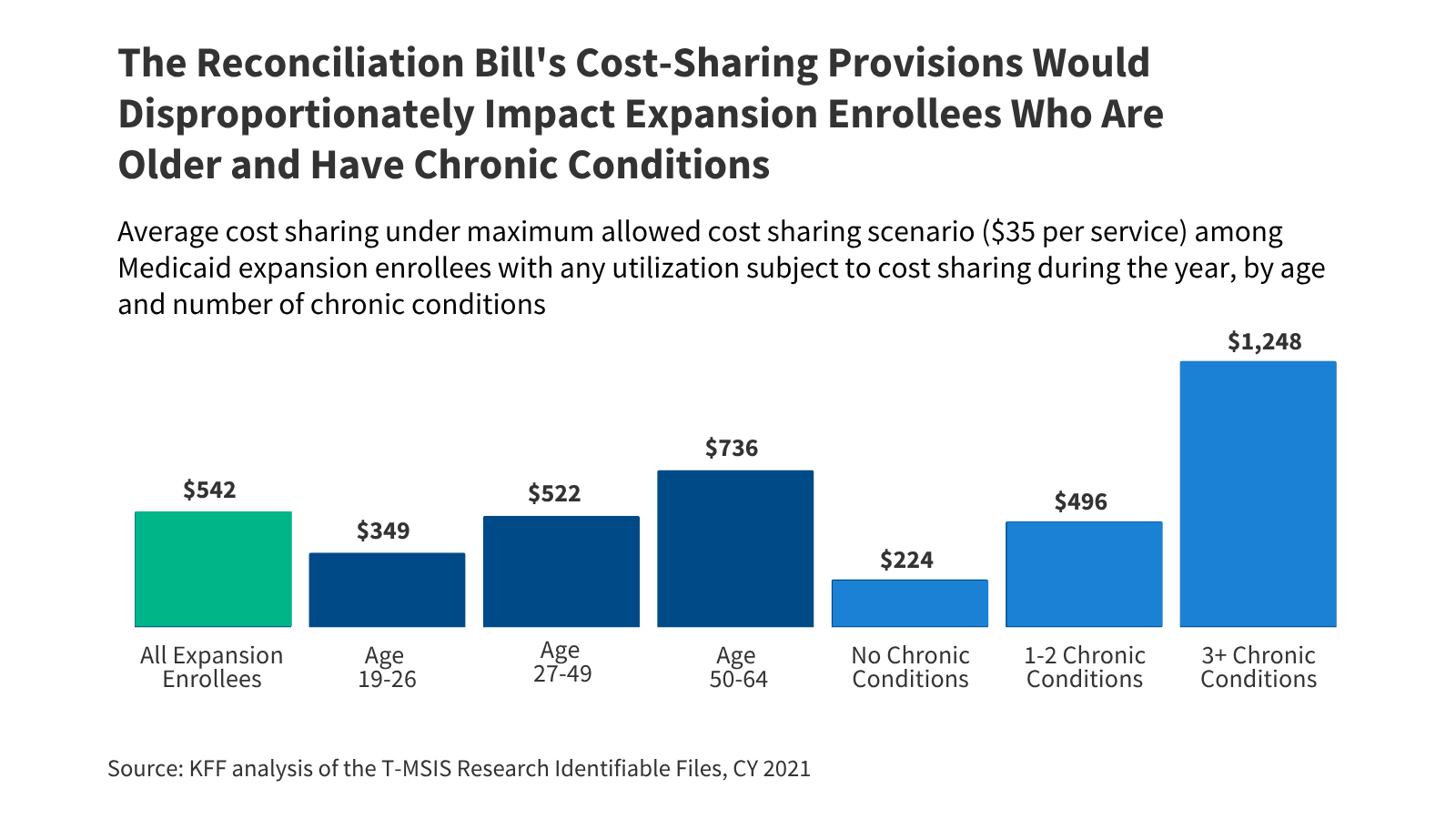
If maximum cost-sharing amounts were imposed, the average expansion enrollee could pay $542 annually for non-exempt services. About 31% of Medicaid expansion enrollees would be exempt due to not using any services or only using exempt services like primary care, mental health treatment, or family planning. Among the remaining enrollees,the average enrollee received 15.5 services and could pay up to $542 per year.

Older expansion adults and those with multiple chronic conditions could face a significantly higher cost-sharing burden. Copayments disproportionately affect enrollees with higher healthcare needs. Adults ages 50-64 could pay an average of $736 per year, one-third more than the average enrollee and more than twice the $349 that younger adults ages 19-26 could pay. Enrollees with three or more chronic conditions could pay up to $1,248 per year, more than twice the average and more than five times what enrollees with no chronic conditions could pay.
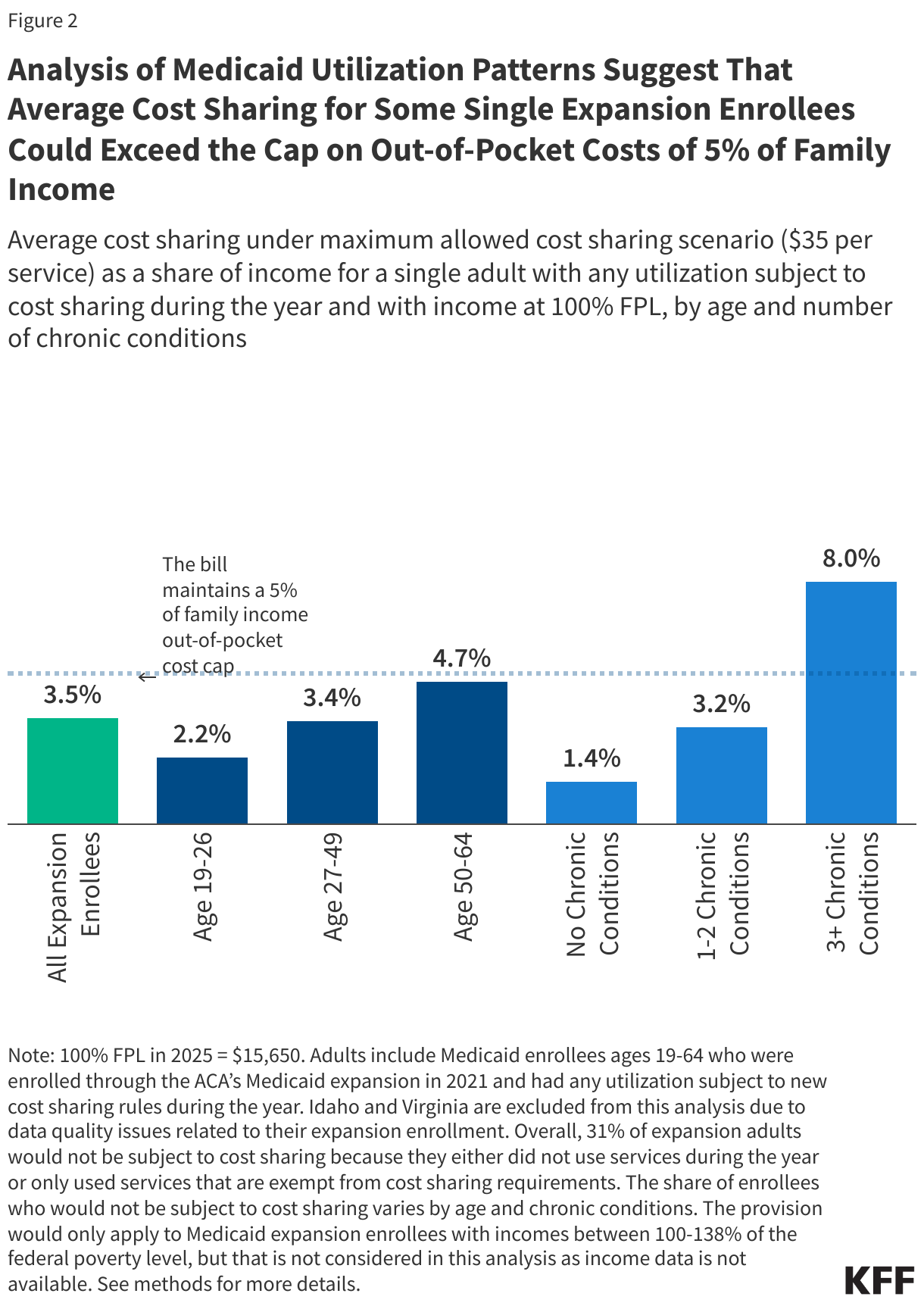
Cost sharing for single Medicaid expansion enrollees ages 50-64 and those with multiple chronic conditions who have income at 100% FPL could approach or exceed the 5% of family income cap on out-of-pocket costs. While cost sharing for many enrollees would remain below the cap, those with high utilization could exceed it. Average cost sharing could reach 4.7% of income for single enrollees ages 50-64 with income at 100% FPL, close to the 5% cap. For single enrollees with three or more chronic conditions, average cost sharing could be 8% of income at 100% FPL, exceeding the cap by three percentage points.
Methods |
|
Medicaid Claims data: This analysis uses the 2021 T-msis Research Identifiable Demographic-Eligibility and Claims Files (T-MSIS data) to identify Medicaid utilization. State Inclusion Criteria: Though Idaho and Virginia expanded Medicaid prior to 2021, adult expansion enrollees primarily show up in the conventional adult eligibility group. Therefore, those expansion states are excluded from this analysis as they do not have sufficient expansion enrollees to be included. Enrollee Inclusion Criteria: Enrollees were included if they were ages 19-64, had Medicaid coverage through the ACA’s Medicaid expansion in an expansion state, and were not dually enrolled in Medicare. Identifying Utilization Subject to Cost Sharing: This analysis identifies eligible health care utilization in T-MSIS by stacking the inpatient (IP) and other services (OT) files, excluding claims that fall into exempted service categories, and then summing the remaining header claims to get a count of claims per enrollee. The prescription drug and institutional long-term care files are excluded from this analysis entirely.After stacking the IP and OT files, the following claims are excluded based on a combination of procedure codes and other methods described in previous KFF work:
The procedure codes used to define these exempted categories are available upon request. Defining Chronic Conditions: This analysis used the CCW algorithm for identifying chronic conditions (updated in 2020). This analysis also included in its definition of chronic conditions substance use disorder,mental health,obesity, HIV, hepatitis Cand intellectual and developmental disabilities. In total, 35 chronic conditions were included. Limitations: The cost sharing provision would only apply to Medicaid expansion enrollees with incomes between 100-138% of the federal poverty level,but that is not considered in this analysis as reliable income data is not available in T-MSIS. Relatedly, this analysis assumes similar utilization patterns across the entire expansion group, which likely does not reflect actual utilization patterns. Expansion enrollees with incomes at 100% or more of the federal poverty level are more likely to work, have fewer chronic conditions, and be younger. Additionally, this analysis assumes a $35 per service cost-sharing level, but it is not clear what cost-sharing states would ultimately levy on services. |
What’s next
The proposed changes are under debate in Congress, and the final impact on Medicaid enrollees will depend on the outcome of these discussions and how states choose to implement any new cost-sharing requirements.