
A rare complication following a minimally invasive procedure to treat a persistent air leak in the lung has been reported, highlighting the potential for unexpected and serious consequences even with established techniques. The case, detailed in a recent report, involved a patient who developed a tension pneumothorax – a life-threatening condition – on both sides of the chest after a unilateral endobronchial valve (EBV) insertion.
Pneumothorax, or collapsed lung, occurs when air leaks into the space between the lung and the chest wall. A persistent air leak is defined as air leakage lasting 5-7 days after the initial event. Traditional treatments include surgical or chemical pleurodesis, procedures aimed at sealing the lung tissue. However, for patients who are not suitable candidates for surgery, or when surgery has failed, EBV insertion offers an alternative. This technique involves placing a one-way valve into the airway to obstruct airflow through the leak, allowing the lung to re-expand.
The case involved a patient with a right-sided pneumothorax who also had a grade 4 glioblastoma, a particularly aggressive form of brain cancer. Surgery was likely contraindicated due to the patient’s underlying condition, making EBV insertion a potentially valuable option. While EBVs have shown promise in managing persistent air leaks, this case underscores the importance of careful monitoring and preparedness for potential complications.
Tension pneumothorax is a particularly dangerous form of pneumothorax where air accumulates in the chest cavity under pressure, compressing the lung and potentially shifting the mediastinum – the space in the chest containing the heart, major blood vessels, and trachea – to the opposite side. This can severely impair breathing and circulation, requiring immediate intervention.
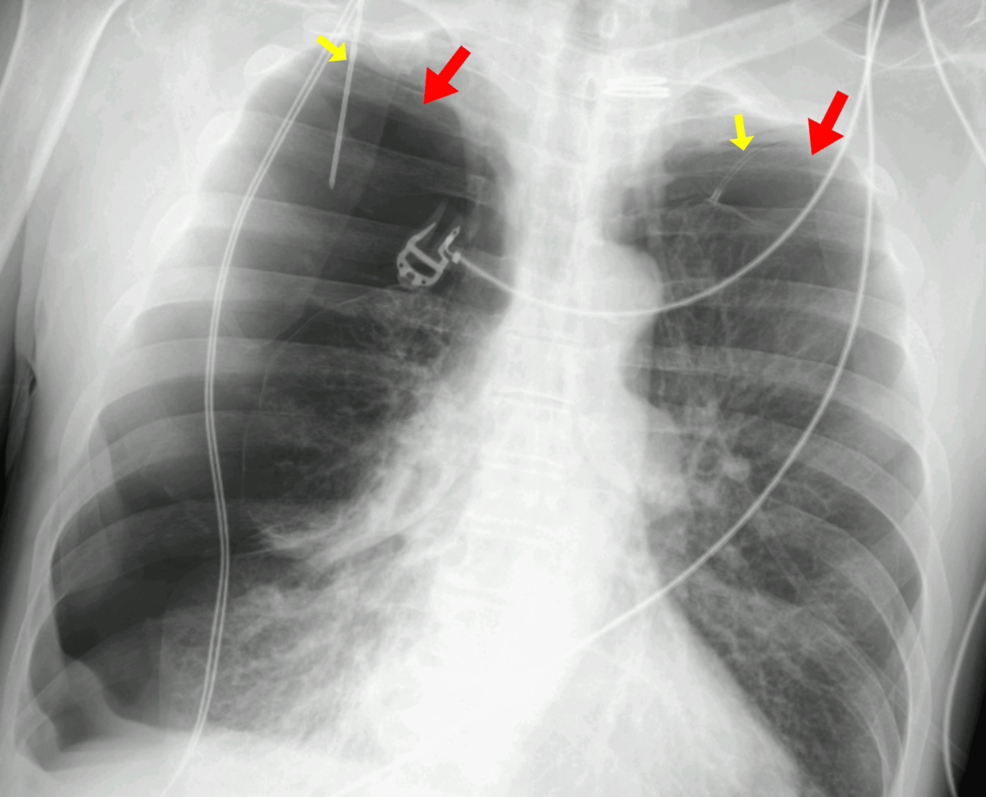
The development of a bilateral tension pneumothorax – meaning on both sides of the chest – following a unilateral EBV placement is exceptionally unusual. The report doesn’t detail the exact mechanism by which this occurred, but it serves as a critical reminder that even well-established procedures carry risks.
Research indicates that pneumothorax itself can lead to prolonged hospital stays and, in some instances, the need to remove the valve and re-expand the affected lung, potentially negating the therapeutic benefit. Pneumothorax is associated with an increased risk of respiratory infections, pneumonia, empyema (a collection of pus in the pleural space), and admission to the intensive care unit (ICU).
Endobronchial valve therapy is often considered for patients with persistent air leaks who have chronic lung disease and are poor surgical candidates. Conventional management often involves prolonged placement of a chest tube, which can be uncomfortable and limit a patient’s mobility. EBVs offer the potential to avoid long-term chest tube dependence, but, as this case illustrates, they are not without risk.
A recent study analyzing patients undergoing endoscopic valve implantation with and without pneumothorax after the procedure assessed emphysema characteristics, collateral ventilation, and patient outcomes. This type of research is crucial for identifying risk factors and improving patient selection for EBV therapy.
Another case highlighted in the available research involved a patient who developed significant hypoxemia – dangerously low blood oxygen levels – after receiving five EBVs. This necessitated the removal of all the valves within 24 hours, demonstrating the importance of close monitoring for signs of respiratory compromise.
While EBV insertion represents a valuable tool in the management of persistent air leaks, healthcare professionals must remain vigilant for potential complications, including the rare but serious possibility of bilateral tension pneumothorax. Careful patient selection, meticulous technique, and prompt recognition and treatment of any adverse events are essential to maximizing the benefits and minimizing the risks of this procedure. Further research is needed to better understand the factors that contribute to complications and to optimize patient outcomes.