
Stroke remains a leading cause of death and disability worldwide, and in India, the burden of this condition is particularly significant. Recent data highlights a concerning trend: in rural areas of India, stroke is now the leading cause of death. This finding, stemming from a population-based study in Ludhiana, underscores the critical need for improved stroke prevention and treatment strategies, particularly in underserved rural communities.
Verbal Autopsy Reveals the Scale of the Problem
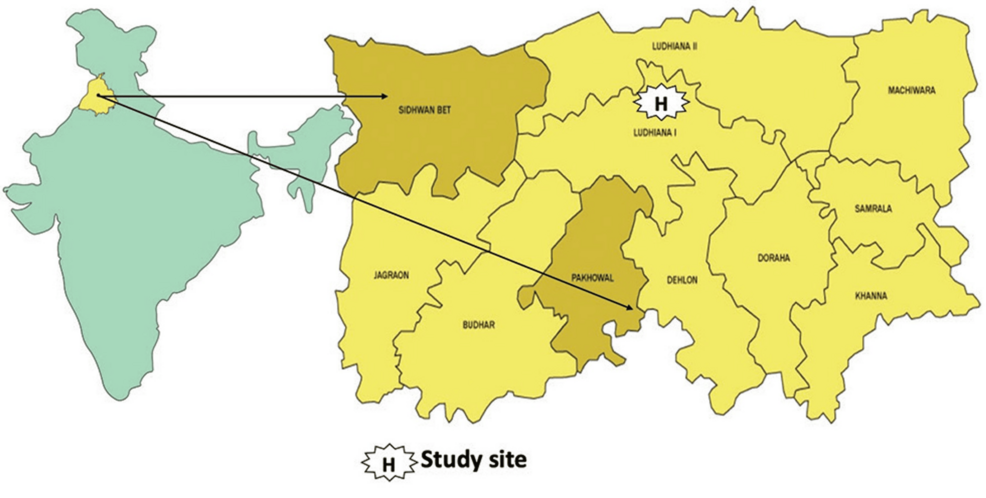
The study, utilizing a “verbal autopsy” approach, analyzed death certificates – including those from hospital deaths and deaths occurring at home – to determine the underlying cause of mortality in the Ludhiana region. This method involves gathering detailed information from family members about the circumstances leading up to a death, allowing trained professionals to assign a probable cause even without a formal medical diagnosis. The results revealed that stroke accounted for the highest number of deaths, surpassing other common causes like heart disease and respiratory infections.
Urban vs. Rural Disparities in Stroke Outcomes
The increased prevalence of stroke as a cause of death in rural areas isn’t an isolated finding. Research consistently demonstrates a significant urban-rural disparity in stroke incidence, risk factors, and outcomes in India. A recent study analyzing data from the SPRINT INDIA trial, a multi-center randomized clinical trial conducted across 31 Indian sites between , and , found that the primary composite outcome – recurrent stroke, high-risk transient ischemic attack (TIA), acute coronary syndrome (ACS), and all-cause mortality – was higher in urban areas compared to rural areas (3.8% vs. 2.4%. p = 0.018) at one-year follow-up. However, it’s important to note that all cases of high-risk TIA occurred in urban participants (p < 0.001).
These seemingly contradictory findings – stroke being the leading cause of death in rural areas while urban areas experiencing a higher rate of recurrent events and TIA – point to complex factors at play. It’s likely that rural populations face greater challenges in accessing timely and effective stroke care, leading to higher mortality rates. Urban areas, while having better access to healthcare, may have a higher prevalence of risk factors contributing to recurrent events.
A Three-Decade Increase in Stroke Incidence
The problem isn’t new. A comprehensive analysis of ischemic stroke in India spanning three decades (1990-2019) reveals a substantial increase in stroke incidence. The study, utilizing data from the Global Burden of Diseases Study, showed an overall increase of 118.8% in stroke incidence during that period. Notably, females experienced a more significant increase in incidence (131.1%) compared to males. This underscores the importance of considering sex-specific risk factors and prevention strategies.
Understanding the Challenges in Rural India
Several factors contribute to the higher stroke burden in rural India. Limited access to healthcare facilities, a shortage of trained medical personnel, and a lack of awareness about stroke symptoms and risk factors all play a role. The SPRINT INDIA trial addressed some of these challenges by implementing a secondary stroke prevention package involving SMS messages, videos, and interactive educational workbooks in 11 Indian languages. However, broader systemic changes are needed to improve stroke care in rural areas.
The rural-urban pattern of stroke incidence and mortality highlights the need for targeted health policy and program planning. Strengthening stroke prevention measures, such as promoting healthy lifestyles, controlling blood pressure and cholesterol, and managing diabetes, is crucial. Equally important is improving access to acute stroke care, including thrombolysis (clot-busting drugs) and mechanical thrombectomy (physical removal of the clot), in rural hospitals.
The Importance of Population-Based Registries
The studies mentioned demonstrate the value of population-based stroke registries in monitoring the burden of stroke and identifying trends. These registries provide a comprehensive surveillance platform to measure stroke incidence, mortality, and outcomes by age, sex, residence, and stroke subtype. The data collected can inform public health interventions and evaluate the effectiveness of stroke prevention and treatment programs.
Further research is needed to fully understand the complex interplay of factors contributing to the urban-rural disparities in stroke outcomes in India. Investigating the specific risk factors prevalent in rural populations, assessing the barriers to accessing stroke care, and evaluating the impact of different intervention strategies are all critical steps towards reducing the burden of stroke in this vulnerable population. The findings from Ludhiana serve as a stark reminder of the urgent need to prioritize stroke prevention and treatment in rural India.