
Accurate diagnosis of Lewy body dementia (LBD), encompassing both dementia with Lewy bodies (DLB) and Parkinson’s disease dementia (PDD), has long been a challenge for clinicians. Misdiagnosis can lead to inappropriate treatment and significantly impact patient care. However, new research published in in Nature Medicine offers a promising advancement: a quantitative biomarker for diagnosing LBD based on levels of the enzyme DOPA decarboxylase (DDC) in cerebrospinal fluid (CSF).
For years, identifying LBD has relied heavily on clinical assessment, which can be subjective and often delayed. Symptoms overlap with other forms of dementia, such as Alzheimer’s disease, making differentiation difficult. Neuroimaging techniques and other fluid biomarkers have shown some promise, but a highly accurate and readily available diagnostic tool has remained elusive. The new study details the development and validation of two DDC immunoassays designed to quantitatively measure DDC levels in CSF.
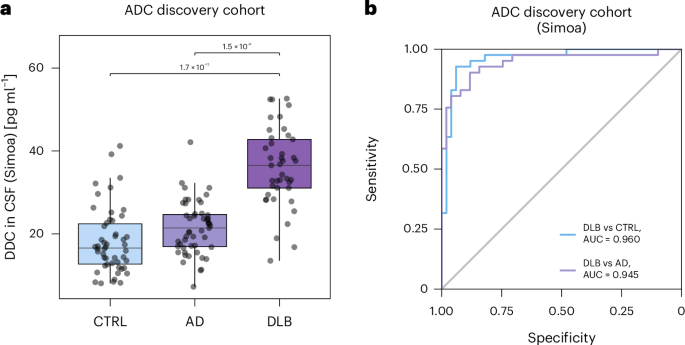
Researchers conducted extensive clinical validation of DDC levels across multiple cohorts, totaling 740 participants. This included a biologically defined cohort of 253 individuals, a cohort of 102 with detailed dopamine transporter imaging, and an autopsy-confirmed cohort of 78. The results demonstrated significantly elevated CSF DDC levels in both DLB and Parkinson’s disease, with levels up to 2.5 times higher compared to healthy controls and 1.9 times higher compared to individuals with Alzheimer’s disease. The assays achieved an area under the curve (AUC) value exceeding 0.9 for differentiating LBD from other neurodegenerative conditions, indicating a high degree of diagnostic accuracy.
The study also explored the relationship between DDC levels and clinical features of LBD. Elevated CSF DDC was associated with the presence of motor impairment, but not with its severity. Interestingly, in autopsy-confirmed DLB cases, higher CSF DDC levels correlated with the progression of α-synuclein pathology, the hallmark protein accumulation characteristic of Lewy body disorders. Further investigation revealed that DDC and α-synuclein colocalized in the substantia nigra of the brain in both DLB and PD patients, suggesting a potential biological link between the two.
DDC’s role in the brain involves the conversion of L-DOPA to dopamine, a neurotransmitter crucial for movement and cognitive function. The increased levels observed in CSF likely reflect neuronal damage and dysfunction associated with the accumulation of α-synuclein. While the precise mechanisms underlying the elevation of DDC in LBD are still being investigated, the findings suggest that DDC is not merely a byproduct of the disease process but may actively contribute to its pathology.
The development of these quantitative DDC immunoassays represents a significant step forward in the diagnosis of LBD. Currently, diagnosis often relies on a combination of clinical symptoms, cognitive testing, and sometimes, dopamine transporter scans. These scans, however, are not always readily available or affordable. A readily accessible CSF biomarker could streamline the diagnostic process, leading to earlier and more accurate diagnoses.
“Accurate diagnosis of dementia with Lewy bodies remains challenging, with misdiagnosis potentially leading to harmful treatment decisions,” researchers noted. The ability to reliably identify LBD early in its course is critical, as the management strategies differ significantly from those used for Alzheimer’s disease. For example, certain antipsychotic medications can worsen symptoms in individuals with LBD, highlighting the importance of a correct diagnosis.
The research team acknowledges that further studies are needed to fully understand the clinical utility of CSF DDC measurements. Ongoing research is focused on determining the optimal timing for CSF sampling, exploring the potential of DDC as a biomarker for predicting disease progression, and investigating whether DDC levels can be used to monitor the response to treatment. The researchers are working to make the DDC immunoassays more widely available to clinical laboratories.
While the findings are promising, it’s important to remember that CSF analysis is an invasive procedure, requiring a lumbar puncture. The decision to perform a lumbar puncture should be made on a case-by-case basis, considering the potential risks and benefits. A single biomarker result should not be used in isolation to make a diagnosis; it should be interpreted in conjunction with clinical findings and other diagnostic tests.
The discovery of DDC as a robust biomarker for LBD builds on previous research identifying it as a potential indicator of both DLB and Parkinson’s disease. Array-based proteomics and mass spectrometry studies conducted in and initially pointed to DDC’s potential, paving the way for the development of these more precise immunoassays. The current study provides compelling evidence supporting DDC’s value in supporting diagnosis and potentially improving patient outcomes.
The development of these new immunoassays offers hope for a future where LBD can be diagnosed more quickly and accurately, leading to more effective treatment and improved quality of life for those affected by these debilitating conditions.