Treatment Challenges for Elderly Multiple Myeloma Patients
As the population ages, the number of patients diagnosed with multiple myeloma, a representative geriatric blood cancer, is on the rise. In fact, the number of domestic patients diagnosed with multiple myeloma has more than doubled in the last decade, exceeding 10,000 individuals as of last year.
Diagnosing multiple myeloma in elderly patients poses a significant challenge due to the overlap of symptoms with existing chronic diseases, making it difficult to detect the disease early. As a result, elderly patients over the age of 70 face limited treatment options, as autologous hematopoietic stem cell transplantation is not possible for this age group, according to domestic medical care benefit standards.
To address this issue, Professor Ho-seop Lee of Kosin University Gospel Hospital emphasized the importance of strategic anti-cancer treatment for elderly patients, taking into consideration factors such as age, co-morbidity, systemic condition, and cognitive function. The treatment strategy often involves a combination of drugs with fewer side effects than the primary treatment given to younger patients, as well as adjusting the dosage and usage based on adverse reactions during treatment.
The Role of VRd Therapy
In clinical practice, VRd (bortezomib + lenalidomide + dexamethasone) therapy is commonly used for elderly patients over 70 years of age. This therapy typically continues for 8 cycles, followed by Rd (lenalidomide + dexamethasone) therapy until disease progression. The National Comprehensive Cancer Network (NCCN) guidelines also recommend VRd therapy as the most strongly preferred therapy for patients in this age group.
However, treatment plans may vary for elderly patients based on their systemic condition and concomitant diseases. Some individuals may receive two-drug therapy with less medication if their systemic condition is relatively poor, while others may opt for lenalidomide monotherapy after discontinuing dexamethasone.
Adapting Treatment Goals
For elderly patients, setting primary treatment goals involves careful consideration of not only the effects of drug treatment but also the quality of life and potential treatment complications. The aim is to avoid overly aggressive treatment, particularly for those with a relatively weak systemic condition.
While autologous hematopoietic stem cell transplantation may not be a primary treatment option for elderly multiple myeloma patients, an individualized and strategic approach to drug treatment is essential to ensure the best possible outcomes while minimizing adverse reactions and maintaining quality of life.
Autologous hematopoietic stem cell transplantation is not possible for patients over 70… Drug treatment is the key
Entered 2023.11.19 09:45 Viewed 1 Entered 2023.11.19 09:45 Viewed 1
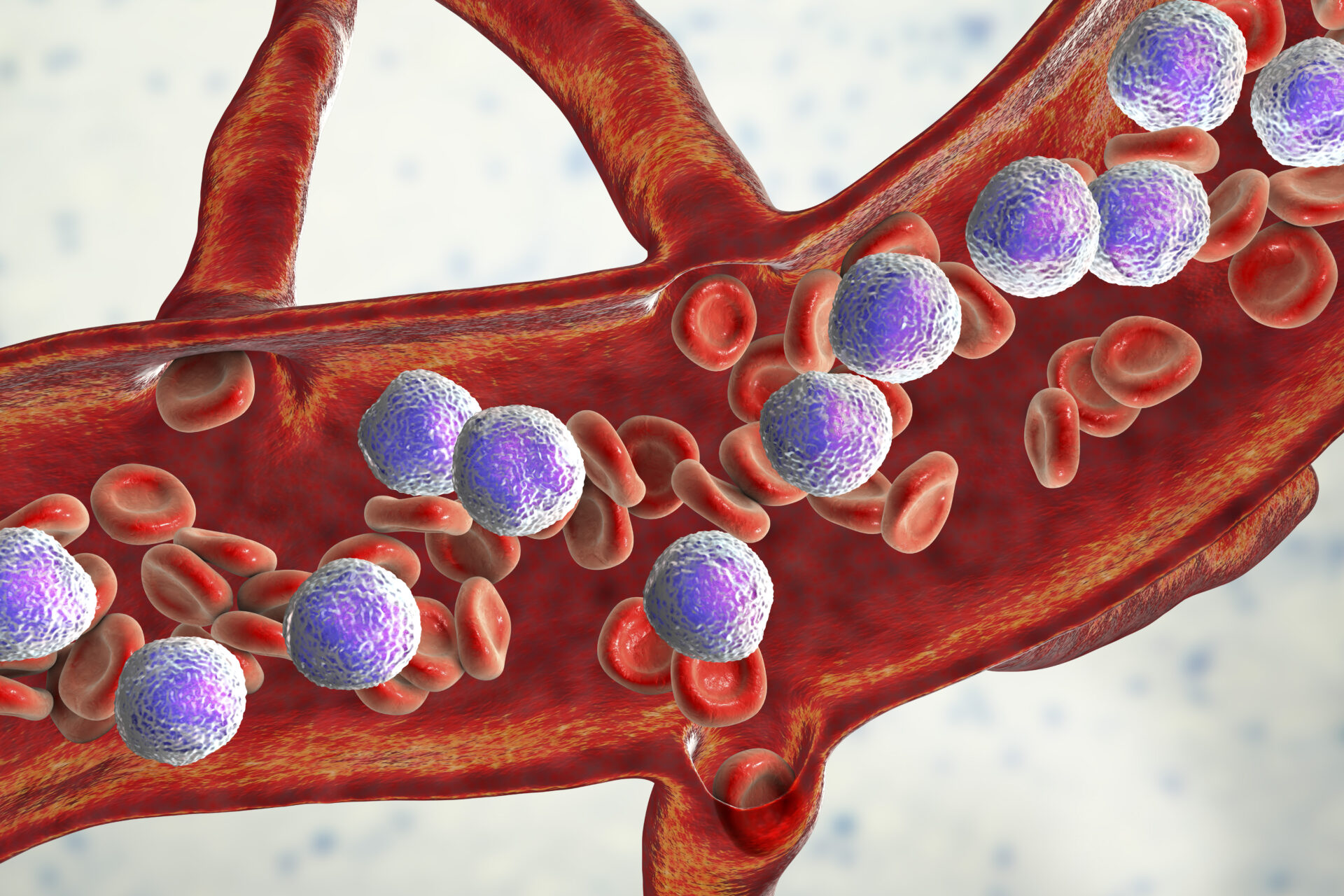
Cancer of the blood. [사진=게티이미지뱅크]This disease, with an onset age of 68 years, is known as a representative geriatric blood cancer. Multiple myeloma, one of the three main blood cancers, is a disease where plasma cells that create immune cells in our body turn into blood cancer and multiply in the bone marrow.
In particular, in Korea, as the population ages, the number of patients increases significantly. As of last year, the number of domestic patients diagnosed with multiple myeloma exceeded 10,000. This figure is more than double compared to 10 years ago (4,658 people).
The early symptoms of multiple myeloma are anemia and fractures, which are common symptoms in everyday life, so it is not easy to detect them early. In addition, as many patients are elderly, they are inevitably accompanied by various chronic diseases such as diabetes, high blood pressure, heart disease, osteoporosis and degenerative arthritis. Accordingly, even if signs of multiple myeloma such as lethargy, fatigue, and edema occur, it is difficult to distinguish them from the symptoms of existing chronic diseases, making it difficult to diagnose elderly patients.
In fact, according to the Health Insurance Review and Assessment Service big data, in 2022, elderly patients (in their 60s to 80s or older) accounted for more than 90% of all multiple myeloma patients. This ratio was reported to be 76.8% in 2012, 10 years ago, and has steadily increased every year since.
To diagnose multiple myeloma, a bone marrow test is performed along with blood and urine tests. At this time, abnormal monoclonal protein (M protein) found in blood or urine is checked, and clonal plasma cells in the bone marrow are checked. If necessary, the diagnosis can be made by imaging tests such as plain radiography (X-ray), computed tomography (CT), and magnetic resonance imaging (MRI), or by tissue examination of the tumor.
Multiple myeloma, which is difficult to diagnose, is not easy to treat either. This is because most patients experience recurrence. In general, multiple myeloma treatment considers the direction of increasing the long-term survival rate by performing ‘autologous hematopoietic stem cell transplantation’ together with anticancer treatment, but the problem is with elderly patients over 70 years old.
As these age groups are not included in the age eligible for transplantation according to the domestic medical care benefit standards, only anticancer treatment is performed without autologous hematopoietic stem cell transplantation. In this regard, from 2022 onwards, elderly patients in their 70s or older who are not eligible for a bone marrow transplant will account for 52%, more than half of all multiple myeloma patients. Moreover, as there are many cases of reduced organ function in these patients, it is essential to consider treatment complications and quality of life.
Professor Ho-seop Lee of Kosin University Gospel Hospital said, “In the case of elderly patients, we strategically conduct anti-cancer treatment based on the Frailty Index, which evaluates age, co-morbidity, systemic condition, and function cognitively comprehensive and classifies them as “fit/moderate/frail.” “We need to establish a treatment strategy,” he said “Usually, a combination of drugs with fewer side effects than the primary treatment given to young patients before autologous hematopoietic stem cell transplantation is used.”
Currently, in clinical practice, anticancer treatment is started with ‘VRd (bortezomib + lenalidomide + dexamethasone)’ therapy for elderly patients over 70 years of age and usually continues for 8 cycles. Thereafter, with the exception of bortezomib, ‘Rd (lenalidomide + dexamethasone)’ therapy will be administered continuously until disease progression.
This treatment direction is also reflected in the National Comprehensive Cancer Network (NCCN) guidelines, which lead the global standard for cancer treatment. For patients in this age group for whom transplantation is not possible, VRd therapy was recommended as the most strongly preferred therapy (category 1).
The Multiple Myeloma Research Group of the Korean Society of Hematology said, “In Korea, patients over the age of 70 are generally not eligible for autologous hematopoietic stem cell transplantation as primary treatment,” adding, “In elderly patients, the medication is reduce it and apply for treatment based on varying criteria according to age.” He said.
“When setting primary treatment goals for elderly patients, it is essential to carefully consider not only the effects of drug treatment but also quality of life and treatment complications,” he said. relatively weak.” “Complications can occur due to overly aggressive treatment,” he explained.
In fact, even among elderly people, if the systemic condition is relatively poor or if there are concomitant diseases, two-drug therapy with less medication is considered rather than three-drug therapy. For example, some elderly patients who are expected to have difficulty tolerating VRd therapy consider starting and maintaining treatment with Rd therapy, which combines two drugs, lenalidomide and dexamethasone, from the beginning.
However, as dexamethasone is a steroid, there is a risk of various side effects such as hypertension and diabetes when administered continuously, so dexamethasone is discontinued after Rd therapy and lenalidomide monotherapy is maintained. In addition, the effectiveness of ‘DRd (daratumumab + lenalidomide + dexamethasone)’ combination therapy for patients who cannot receive a transplant has been confirmed in clinical studies.
Professor Ho-seop Lee said, “For elderly multiple myeloma patients, autologous hematopoietic stem cell transplantation has been ruled out as a primary treatment option, so it is important to understand the patient’s condition well and set the initial treatment plan accordingly. strategic.” He added, “According to adverse reactions that occur during the treatment, active treatment is recommended “The dose and use must be adjusted accordingly,” he emphasized.
#Multiple #myeloma #doubles #years.. #ten #people